Reinventing rural health care
Health care delivery faces challenges in ND, other nearby states

Submitted Photo Chandra Flammang, a medical technologist in Trinity Hospital Laboratory’s Microbiology Section in Minot, examines a specimen using a high resolution microscope. Trinity Health, including Trinity Hospital, provides regional health care to people of North Dakota and eastern Montana. Some area rural hospitals are designated critical access hospitals
Rightsizing health care services to fit community needs is one of four specific areas identified in a new report on the challenges of health care delivery in rural areas of North Dakota and six other states in the Upper Midwest.
The Bipartisan Policy Center based in Washington, D.C., recently released the report, “Reinventing Rural Health Care: A Case Study of Seven Upper Midwest States.”
The report was created over a six-month period in collaboration with the Center for Outcomes Research and Education with insight from nearly 100 regional and national thought leaders plus roundtables held with health care providers from the seven states. The work was financed by a grant from The Leona M. and Harry B. Helmsley Charitable Trust.
Health care professionals from North Dakota participating in round tables or personal interviews for the project included Darrold Bertsch, CEO of Sakakawea Medical Center, Hazen; and John Kutch, president/CEO of Trinity Health, Minot. Bertsch was also one of four rural health panelists at the report roll-out in Washington, D.C.
According to the new report, Centers for Disease Control and Prevention data shows:
Submitted Photo Michael Wentz, a medical technologist in Trinity Hospital Laboratory’s Microbiology Section in Minot, places a specimen on a plate of agar, a growth medium used to culture microorganisms.Trinity Health, including Trinity Hospital, provides regional health care to people of North Dakota and eastern Montana. Some area rural hospitals are designated critical access hospitals.
® Forty-six million Americans living in rural areas are at a greater risk of dying from heart disease, cancer, chronic lower respiratory disease, and stroke than their urban counterparts.
® Rural residents have higher rates of obesity, tobacco and opioid use, and suicide than those living in urban areas.
The Bipartisan Policy Center’s findings from the seven Upper Midwest states identified four specific policy areas for developing recommendations. The four key areas for reform could apply nationally to all rural communities.
They are:
® Rightsizing Health Care Services to Fit Community Needs. Recognizing not every community needs a Critical Access Hospital, communities should adjust services to better suit the needs of the local area. In an effort to prevent closures, Critical Access Hospitals should be allowed to provide more primary care and prevention focused services.

Deanna Miller, a certified pharmacy technician in Trinity Hospital’s Pharmacy Department, scans a unit of medication before entering it into the department’s automated dispensing system. Trinity Health, including Trinity Hospital, provides regional health care to people of North Dakota and eastern Montana. Some area rural hospitals are critical access hospitals. Submitted Photo
® Creating Rural Funding Mechanisms. Given small population sizes, growing health care needs, and demographic trends, rural areas need alternative Medicare and Medicaid reimbursement metrics and payment mechanisms that allow for value-based alternative payments models and innovation. Appropriate reimbursement mechanisms for telemedicine should also be examined to accommodate the virtual provider and the on-site provider or host hospital.
® Building and Supporting the Primary Care Physician Workforce. New workforce models should be examined in collaboration with universities and residencies to expose providers to rural environments and telemedicine, and reserve placements in medical programs for rural residents. Alternative providers such as nurse practitioners and physician assistants can fill vital primary care roles in rural communities.
® Expanding Telemedicine Services. Telemedicine is a promising way to connect patients with providers and create a peer network for rural providers that will improve recruitment and retention. However, it must be supported by adequate broadband services and reimbursement. Rural health systems need to provide health professionals with the necessary tools and technology to offer this type of quality care to their patients.
At the unveiling of the report, Sen. Heidi Heitkamp, co-chair of the Rural Health Caucus, said it’s “virtually impossible to have a real meaningful discussion about rural healthcare without talking about the issues of rural America,” naming higher poverty rates, more isolation, less transportation and an aging population.
“And now we have challenges in the ag economy with low commodity prices and in our states a growing concern about drought which is huge. So I don’ think that we can really talk about health care unless we can talk about meeting all the challenges of rural America,” she said.
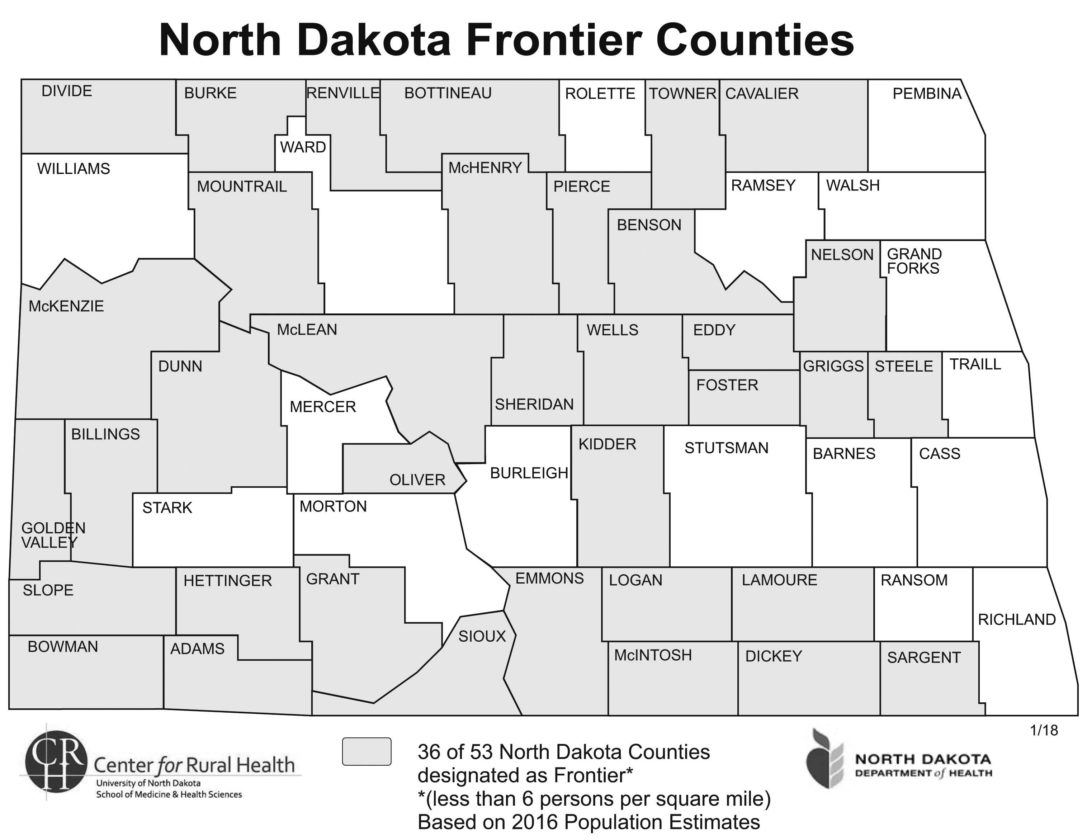
Submitted Art This map from the Center for Rural Health at the University of North Dakota School of Medicine and Health Sciences show the 36 North Dakota counties designated as “frontier” or those with less than six people per square mile according to the 2016 population estimates.
On top of that, she said when you look at private employment in North Dakota basically the largest private employer in a state like North Dakota is in health care.
“So not only do we have the challenges of rural health care, we know how critically important providing that health care is to the economy of our state and you’ll see that all across the region on the states that you’ve identified,” she said.
Heitkamp said one of the frustrations she has with how policy issues are dealt with in Washington, D.C., is that they revisit the same issues over and over again. She said she could go through a whole list of items and if all of them were fixed it would be a good thing. “But it won’t solve the problem of dealing with rural healthcare and that’s why the work of this commission and committee is so critical. That’s why we want to thank the Helmsley Foundation for focusing on rural health care because it’s hard to get foundations to really focus on places like ours, like North Dakota.
Heitkamp said the right challenges were identified in the new study. “But I think we need to be driving a proactive strategy in rural health care needs,” she said. She said there should be talks about systemic change, fighting for a different way of delivery and paying for health care services in rural America.
Heitkamp, a Democrat, and Republican Sen. Pat Roberts of Kansas introduced a bill to fund the state offices of Rural Health grant program.
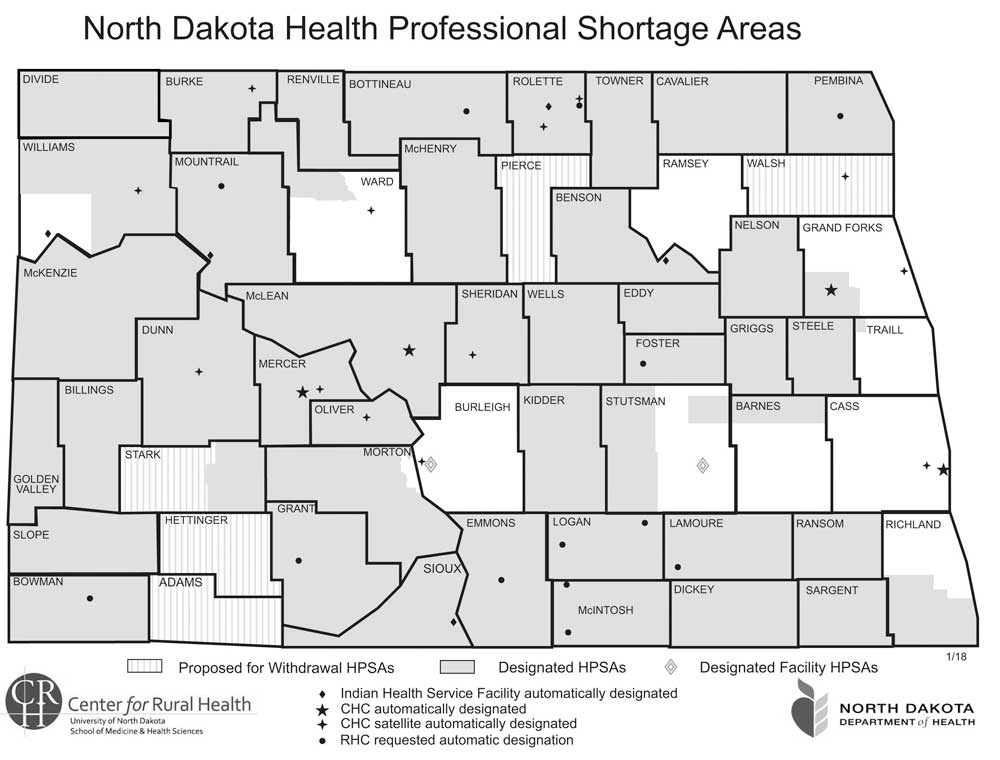
Submitted Art This map from the Center for Rural Health at the University of North Dakota School of Medicine and Health Sciences shows the North Dakota counties with a shortage of health professionals. The “gooseneck area” of Ward County is included in the area.
The full report and executive summary can be viewed at: bipartisanpolicy.org/press-release/bpc-report-rightsizing-rural-health-care-in-america-demands-national-attention
–
Some rural health facts
• Thirty-six of North Dakota’s 53 counties are designated as “frontier” with less than six persons per square mile. Less than two people per square mile live in some areas.
• There are only 36 critical access hospitals in North Dakota.
• Forty of North Dakota’s 53 counties are designated as Health Professional Shortage Areas.
Source: Rural Health Information Hub
–
Area critical access hospital locations
• Carrington Health Center, Carrington, 25 beds.
• Community Memorial Hospital, Turtle Lake, 25 beds.
• Garrison Memorial Hospital, Garrison, 22 beds.
• Heart of America Medical Center, Rugby, 25 beds.
• Kenmare Community Hospital, Kenmare, 25 beds.
• McKenzie County Memorial Hospital, Watford City, 24 beds.
• Mercy Hospital, Devils Lake, 25 beds.
• Mercy Medical Center, Williston, 25 beds.
• Mountrail County Medical Center, Stanley, 11 beds.
• Presentation Medical Center, Rolla, 25 beds.
• Sakakawea Medical Center, Hazen, 25 beds.
• St. Aloisius Medical Center, Harvey, 25 beds.
• St. Andrews Health Center, Bottineau, 25 beds.
-

- Submitted Photo Chandra Flammang, a medical technologist in Trinity Hospital Laboratory’s Microbiology Section in Minot, examines a specimen using a high resolution microscope. Trinity Health, including Trinity Hospital, provides regional health care to people of North Dakota and eastern Montana. Some area rural hospitals are designated critical access hospitals
-

- Submitted Photo Michael Wentz, a medical technologist in Trinity Hospital Laboratory’s Microbiology Section in Minot, places a specimen on a plate of agar, a growth medium used to culture microorganisms.Trinity Health, including Trinity Hospital, provides regional health care to people of North Dakota and eastern Montana. Some area rural hospitals are designated critical access hospitals.
-

- Deanna Miller, a certified pharmacy technician in Trinity Hospital’s Pharmacy Department, scans a unit of medication before entering it into the department’s automated dispensing system. Trinity Health, including Trinity Hospital, provides regional health care to people of North Dakota and eastern Montana. Some area rural hospitals are critical access hospitals. Submitted Photo
-

- Submitted Art This map from the Center for Rural Health at the University of North Dakota School of Medicine and Health Sciences show the 36 North Dakota counties designated as “frontier” or those with less than six people per square mile according to the 2016 population estimates.
-

- Submitted Art This map from the Center for Rural Health at the University of North Dakota School of Medicine and Health Sciences shows the North Dakota counties with a shortage of health professionals. The “gooseneck area” of Ward County is included in the area.
• St. Luke’s Hospital, Crosby, 25 beds.
• Tioga Medical Center, Tioga, 25 beds.
• Towner County Medical Center, Cando, 20 beds.
Source: Flex Monitoring Team. Updated Jan. 12, 2018.
Local News
Missionaries to speak at Minot Baptist
Patrick and Victoria Weimer, missionaries to Iceland as pioneer church planters since 1997, will be speaking at ...
US 52 work to affect several communities
Work on U.S. 52 that is expected to begin May 4 will affect Harvey, Drake, Anamoose, Martin and Fessenden, ...

Governor tours Minot’s flood construction
Police officer struck by vehicle
The Minot Police Department is investigating an incident on Wednesday evening which resulted in a police officer ...

Parties in shooting case await Supreme Court ruling
